Intro
Conception is often described as a single moment, but biologically it is a coordinated sequence of events involving the menstrual cycle, ovulation, sperm transport, fertilization, early embryonic cell division, and implantation. Each step depends on timing, hormone signaling, tubal function, sperm quality, and a receptive uterine lining.
Understanding how conception happens can be reassuring, especially if you are trying to become pregnant, planning ahead, or making sense of early pregnancy testing. The steps below explain the process in medically accurate terms while acknowledging that real bodies do not always follow textbook timing. If you have concerns about fertility, cycle irregularity, pain, bleeding, or pregnancy symptoms, a qualified healthcare professional can help interpret your individual situation.
Highlights
Conception begins within the context of the menstrual cycle, with the first day of bleeding counted as day one of a new cycle.
Ovulation typically occurs around the middle of a 28-day cycle, but timing varies; the egg can usually be fertilized for about 12 to 24 hours after release.
Sperm must travel through the cervix and uterus into the fallopian tube, where fertilization most commonly occurs.
After fertilization, the zygote divides repeatedly, becomes a blastocyst, and reaches the uterus before implantation.
Implantation triggers hormone signals such as human chorionic gonadotropin, or hCG, which pregnancy tests are designed to detect.
1. The cycle begins: the body prepares for a possible pregnancy
The first day of a menstrual period is counted as day one of the . During the early part of the cycle, the brain and ovaries communicate through hormones, especially follicle-stimulating hormone, or FSH, and luteinizing hormone, or LH. FSH helps ovarian follicles grow. Each follicle contains an immature egg, but one follicle becomes dominant and continues developing.
As the dominant follicle matures, it produces estrogen. Rising estrogen helps thicken the endometrium, the lining of the uterus, creating a more suitable environment in case an embryo implants later. Estrogen also changes , making it more slippery, stretchy, and sperm-friendly around the .
Although many explanations use a 28-day cycle with around day 14, this is an average, not a rule. Some people ovulate earlier or later, and cycle length can vary due to stress, illness, age, weight changes, lactation, medications, polycystic ovary syndrome, thyroid disease, and other factors. If cycles are very irregular or absent, professional evaluation may be helpful.
2. Ovulation: the egg is released
a surge in luteinizing hormone prompts the dominant ovarian follicle to rupture and release a mature egg, also called an oocyte. In a typical 28-day cycle, this often occurs near day 14. However, the on the individual rather ]] the calendar alone.
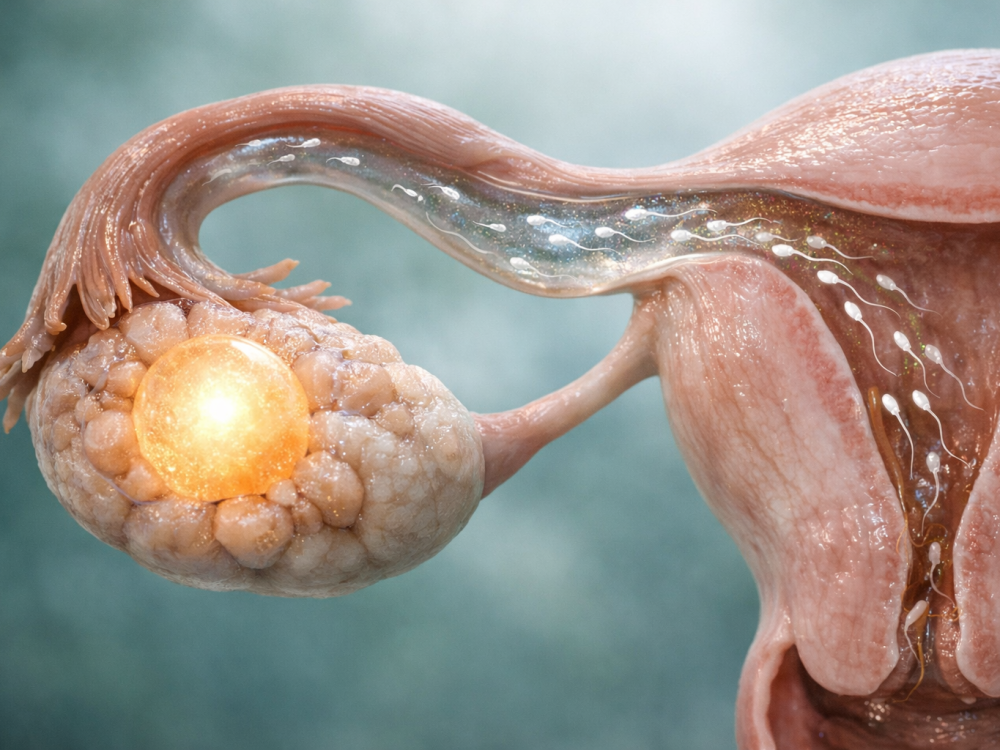
Once released, the egg float randomly through the abdomen. Fingerlike projections at the end of the fallopian tube, called fimbriae, help sweep the egg toward the tube. Tiny hairlike structures called cilia, along gentle muscular contractions of the fallopian tube, move the egg inward. UCSF Heh describes egg transport through the tube as a process involving fimbrial capture, ciliary movement, and muscular activity, with egg transport taking about 30 hours.
The egg has a limited period during is possible, generally about 12 to 24 hours . Sperm, in the reproductive tract under favorable conditions, often several. This is why in the can still lead to pregnancy.
3. Sperm transport: reaching the fertilization site
After ejaculation in the vagina, sperm must pass through the cervix, cross the uterine cavity, and enter the fallopian tube. This journey is demanding. Vaginal acidity, quality, uterine contractions, immune defenses, and sperm motility all influence how many sperm progress. Although millions of sperm may be ejaculated, only a small fraction reach the upper reproductive tract.
Around , estrogen-dominant cervical mucus becomes thinner and more elastic, which can help sperm movement. Sperm also undergo capacitation, a series of biochemical changes inside the female reproductive tract that improves their ability to penetrate the egg’s outer layers. Without capacitation, sperm generally cannot fertilize the egg.
Fertilization usually occurs in the ampulla, the wider outer portion of the fallopian tube. Timing is crucial: the egg and sperm must be present in the tube at approximately the same time. This timing explains why the includes the days before as well as day itself.
4. Fertilization: one sperm enters the egg
Fertilization is the union of sperm and egg. The egg is surrounded by protective layers, including the corona radiata and the zona pellucida. Sperm release enzymes and use motility to help penetrate these layers. Typically, only one sperm successfully fuses with the egg’s membrane.
Once one sperm enters, the egg activates mechanisms that prevent additional sperm from entering, a process that helps avoid polyspermy, or fertilization by more than one sperm. The genetic material from the egg and sperm then combines, forming a single cell called a zygote. This zygote contains the full complement of chromosomes needed to guide early development.
At this stage, chromosomal sex is also determined by the sperm contribution: an X-bearing sperm results in an XX embryo, while a Y-bearing sperm results in an XY embryo. However, it is important to remember that biological sex development is complex, and variations in chromosomes, hormones, or anatomy can occur.
5. Early cell division: from zygote to blastocyst
After fertilization, the zygote begins cleavage, a series of rapid cell divisions. The total size of the early embryo does not increase much at first; instead, one cell divides into two, then four, then eight, and so on. Over the next several days, the developing embryo continues traveling through the fallopian tube toward the uterus.
By about three to four days after fertilization, the embryo may reach a compacted stage called a morula. As development continues, a fluid-filled cavity forms, and the embryo becomes a blastocyst. By the time it reaches the uterus, it may contain around 100 cells. The blastocyst has an inner cell mass, which contributes to the embryo, and an outer cell layer, which contributes to the placenta and supporting tissues.
This early journey is delicate. The fallopian tube must be open and functioning, and coordinated ciliary and muscular movement must help transport the embryo. If an embryo implants outside the uterus, most commonly in a fallopian tube, this is an ectopic pregnancy, which can be dangerous and requires urgent care.
6. Implantation: the blastocyst attaches to the uterine lining
Implantation usually begins about six fertilization, hough timing varies. The blastocyst first sheds its outer shell, a process times called hatching. It then attaches to the endometrium and begins embedding into the uterine lining. For implantation to proceed, the endometrium must be hormonally prepared and receptive.
The outer trophoblast cells of the blastocyst begin interacting maternal tissue and contribute to early placental development. These cells start producing human chorionic gonadotropin, commonly called hCG. hCG helps maintain the corpus luteum in the ovary, which continues producing progesterone. Progesterone supports the uterine lining and helps maintain early pregnancy.
Some people notice light spotting or mild cramping around the time of implantation, but many notice nothing at all. Implantation symptoms are not a reliable way to confirm pregnancy because they can resemble normal premenstrual changes. A needed, clinical evaluation provide more dependable information.
7. Pregnancy testing and very early development
Home pregnancy tests detect hCG in urine. Because hCG rises implantation, testing too early may produce a negative result even if conception has occurred. Many tests are most reliable after a missed period, though sensitivity varies by product and . Blood tests ordered by a clinician can detect and quantify hCG earlier and more precisely than most urine tests.
After implantation, embryonic development continues quickly. In the early weeks, the gestational sac, yolk sac, embryo, and cardiac activity become visible on ultrasound in a predictable but variable sequence. Dating is usually based on the first day of the last menstrual period, not the day of fertilization, because is often uncertain. This is why a pregnancy counted as four weeks gestational age is typically only about two weeks after fertilization.
If you have a positive pregnancy test, severe one-sided pelvic pain, er pain, fainting, heavy bleeding, or significant dizziness, seek urgent medical care, as these can be warning signs of ectopic pregnancy or other serious conditions. If you are and have questions about , chronic conditions, prenatal vitamins, or prior pregnancy losses, a clinician can help you plan safely.
8. Why conception timing varies from person to person
The step-by-step sequence is consistent in broad outline, but the timing is not identical for everyone. may shift from cycle to cycle, especially during adolescence, perimenopause, postpartum periods, breastfeeding, after stopping hormonal contraception, or during periods of physiological stress. Medical conditions such as endometriosis, fibroids, pelvic inflammatory , thyroid disorders, hyperprolactinemia, or polycystic ovary syndrome can also affect .
can bring excitement, uncertainty, and emotional strain. Many couples conceive within several months, but it is also common for to happen immediately. In general, people under 35 are often advised to seek after 12 months of regular unprotected ]] ; people 35 or older are often advised to seek after six months. Earlier consultation is reasonable if are very irregular, there is known reproductive , prior pelvic surgery, loss, or concerns about sperm factors.
Because both partners’ reproductive , may include assessment, tubal and uterine , hormone testing, review of medications and history, and semen analysis. A recommendations to age, history, goals, and risk factors.
When to seek medical advice urgently
- Seek urgent care for severe pelvic or abdominal pain, fainting, shoulder pain, or heavy bleeding after a positive pregnancy test.
- Contact a clinician if you have a positive pregnancy test and a history of ectopic pregnancy, tubal surgery, or significant pelvic infection.
- Ask for medical guidance before stopping or starting medications while trying to conceive or after a positive test.
- Consult a healthcare professional if menstrual cycles are absent, very irregular, or associated with severe pain.
- If pregnancy has not occurred after the recommended trying period for your age and history, consider a fertility evaluation.
Tools & Assistance
- Menstrual cycle and ovulation tracking with dates, bleeding patterns, and symptoms
- Preconception visit with an obstetrician-gynecologist, midwife, or primary care clinician
- Home pregnancy test used according to package timing and instructions
- Fertility clinic consultation when conception is delayed or risk factors are present
- Urgent care or emergency services for symptoms concerning for ectopic pregnancy or heavy bleeding
FAQ
When exactly does conception happen?
Conception is commonly used to mean fertilization, when sperm and egg unite, usually in the fallopian tube within about 24 hours after ovulation. Some clinicians and sources discuss conception as a broader process that includes implantation.
Can conception happen days after sex?
Yes. Sperm can survive for several days in fertile cervical mucus, so intercourse before ovulation can lead to fertilization when the egg is released.
How soon after conception can a pregnancy test be positive?
Pregnancy tests detect hCG, which rises after implantation, not immediately after fertilization. Many urine tests are most reliable after a missed period, though timing and sensitivity vary.
Is implantation bleeding necessary for pregnancy?
No. Some people report light spotting around implantation, but many have no noticeable symptoms. Spotting can also have other causes, so persistent, painful, or heavy bleeding should be discussed with a clinician.
Does ovulation always happen on day 14?
No. Day 14 is a useful example for a 28-day cycle, but ovulation varies between people and from cycle to cycle. Tracking patterns can help, but medical advice is best for irregular cycles.
Sources
- Cleveland Clinic — Conception: Fertilization, Process & When It Happens
- UCSF Health — Conception: How It Works
- WebMD — Conception: From Egg to Embryo Slideshow - Pregnancy
Disclaimer
This article is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Consult a qualified healthcare professional for personal guidance about fertility, pregnancy, symptoms, or medical conditions.















