Intro
Week 3 of pregnancy is a biologically remarkable moment, even though many people do not yet know they are pregnant. In standard pregnancy dating, week 3 is counted from the first day of the last menstrual period, which means conception often occurs around this time, roughly two weeks after that period began. At the cellular level, a sperm and egg may meet, genetic material combines, and the first stages of embryonic development begin.
This week can feel emotionally complex: hopeful, uncertain, or invisible because there may be no clear symptoms yet. Understanding what is happening inside the body can make the waiting period feel less mysterious. The information below explains fertilization, the early journey through the fallopian tube, blastocyst formation, implantation, and when pregnancy hormones may begin to rise, while emphasizing that individual timing varies and personal medical questions are best discussed with a qualified healthcare professional.
Highlights
Week 3 is commonly when fertilization occurs, creating a zygote with a full set of 46 chromosomes.
The fertilized egg divides rapidly as it travels through the fallopian tube toward the uterus.
By the end of this early sequence, the developing structure becomes a blastocyst, with cells destined to form the embryo and placenta.
Implantation usually begins after the blastocyst reaches the uterine lining, often around the transition from week 3 to week 4.
Most people have few or no pregnancy symptoms at this stage, and home pregnancy tests may still be negative until hCG rises enough to detect.
Why week 3 is often the week of conception
Pregnancy is usually dated from the day of the ]], not from the exact day of fertilization. This convention is used because the menstrual period is usually easier to identify than or . In a typical 28-day cycle, occurs around day 14, and fertilization may occur within about 24 hours after the egg is released if sperm are present in the reproductive tract.
Because of this dating method, a person who is 3 s pregnant by obstetric dating may have only just conceived. This can feel counterintuitive: ly, pregnancy is already counted as several s along before an has implanted or before a pregnancy test turns . Cycle length, timing, brefeeding, recent hormonal contraception, polycystic ovary syndrome, perimenopause, and fertility treatments can all shift the timeline.
If you are tracking , using assisted reproduction, or have irregular cycles, your clinician may use findings, data, transfer date, or laboratory results to refine dating later. At 3, however, the main developmental theme is the beginning of a new genetic individual at the cellular level.
Fertilization: the formation of the zygote
Fertilization usually occurs in the fallopian tube, most often in the ampulla, the wider outer portion of the tube. A single sperm penetrates the outer layers of the egg, and the egg’s membrane changes to help prevent additional sperm from entering. The sperm and egg each contribute 23 chromosomes, creating a one-cell zygote with 46 chromosomes.
These chromosomes carry the genetic instructions that influence biological sex, eye color, blood type, and many aspects of development. At this point, the new cell is microscopic and not yet connected to the parent’s bloodstream. Nutritional and hormonal support comes from the local reproductive environment as the zygote begins its first divisions.
Within roughly a day after fertilization, cleavage divisions begin. These are rapid mitotic divisions in which the single cell becomes two, then four, then eight cells, without a major increase in overall size. The developing structure remains enclosed within the zona pellucida, a protective glycoprotein shell that helps guide early development and prevents premature implantation inside the fallopian tube.
From zygote to morula: early cell division during the journey to the uterus
As the travels through the fallopian tube toward the uterine cavity, it continues to divide. Around three to four days after fertilization, it may become a morula, a compact ball of cells. The term morula comes from the Latin word for mulberry, reflecting its clustered appearance under a microscope.
This journey depends on coordinated movement from tiny hair-like cilia lining the fallopian tube and gentle muscular contractions. The timing matters: the needs to arrive in the uterus when the endometrium, or uterine lining, is receptive. Hormones from the ovarian corpus luteum, especially progesterone, help prepare and maintain this lining.
Most cannot feel these events. Cramping, discharge changes, bre tenderness, or mood shifts during this time are more related to normal luteal-phase hormone changes than to a confirmed pregnancy. Still, every body is different, and symptoms alone cannot reliably confirm or exclude pregnancy at week 3.
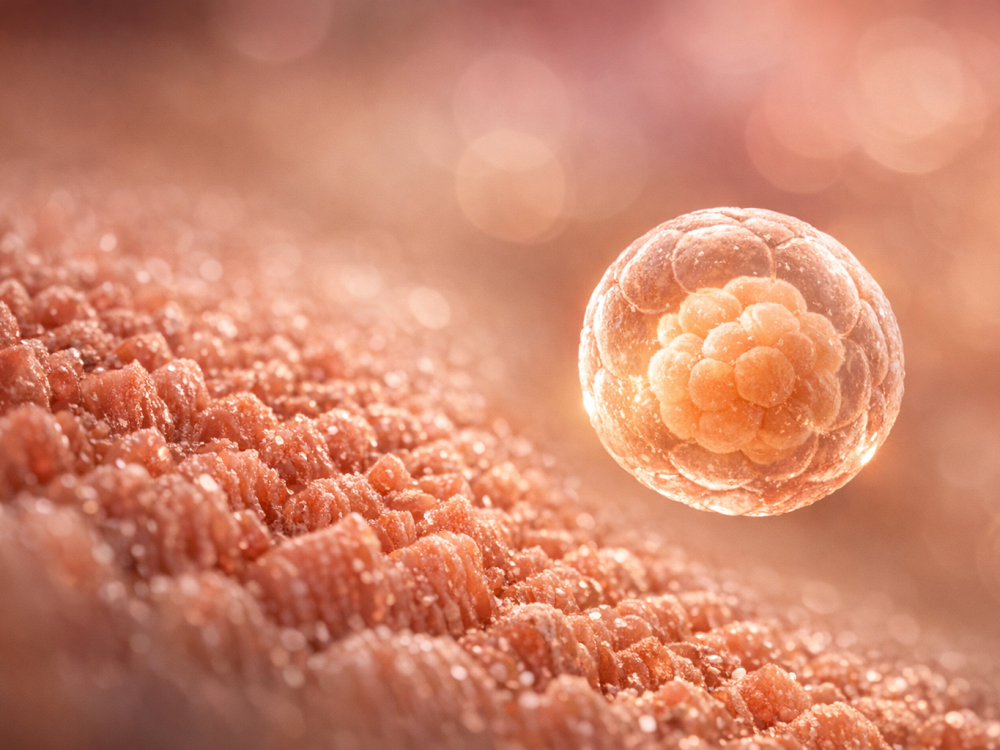
Blastocyst formation: the first specialization of cells
By about five days after fertilization, the morula develops into a blastocyst. This is a fluid-filled structure with two important cell populations. The inner cell mass, also called the blast, will contribute to the . The outer cell layer, called the trophoblast, will contribute to the placenta and supporting structures.
The blastocyst also begins to hatch from the zona pellucida. Hatching is important because the blastocyst must directly contact the uterine lining to implant. Without this step, it cannot properly attach to the endometrium.
At this stage, the future embryo is still extremely small, but differentiation has begun. The amniotic sac and early placental tissues will start forming in the days that follow. The placenta is not yet mature, but its earliest cellular foundations are being established, eventually allowing oxygen, nutrients, and waste products to move between maternal and fetal circulations without the two blood supplies normally mixing directly.
Implantation: when the blastocyst meets the uterine lining
typically begins after the blocyst reaches the uterus, often around six to ten days after fertilization, which may fall near the end of week 3 or during week 4 depending on timing. The trophoblast adheres to the endometrial surface and then invades into the lining. This process is highly regulated by molecular signals between the blastocyst and the endometrium.
As progresses, trophoblast cells begin to differentiate into layers that help form the placenta. These cells also start producing human chorionic gonadotropin, commonly abbreviated hCG. hCG signals the corpus luteum to continue producing progesterone, which supports the uterine lining and early pregnancy.
Some notice very light spotting around the time of implantation, but many do not. Implantation , when it occurs, is usually lighter than a period. However, bleeding patterns vary widely, and bleeding can have many causes. Heavy bleeding, severe pain, dizziness, er pain, or fainting should be discussed urgently with a healthcare professional, because they may indicate a problem that needs prompt evaluation.
Early embryo development and the beginning of pregnancy hormones
Once implantation begins, the and its supporting tissues enter a phase of rapid organization. The inner cell mass will soon organize into layers that give rise to all major tissues and organs. The amniotic cavity begins to develop, and placental structures expand. This is still far before organs are visibly formed, but the groundwork for later development is being laid.
hCG is the hormone detected by most home pregnancy tests. In the earliest days implantation, hCG may be too low to detect in urine. Blood tests can sometimes detect hCG earlier than urine tests, but interpretation depends on timing, the laboratory assay, and clinical context. A negative test at 3 does not necessarily mean pregnancy has not occurred, especially if testing happens before or soon implantation.
If you are undergoing fertility treatment, clinic may advise specific timing for serum hCG testing and may caution against testing too because of false negatives or confusion from medications. If you conceived out treatment, testing a generally gives more reliable home results than testing in the middle of ]] 3.
What you may feel during week 3
Many people feel exactly the same as they do in any other cycle. Others notice nonspecific symptoms overlap with premenstrual symptoms. These can include mild pelvic twinges, breast tenderness, bloating, fatigue, increased cervical mucus, mood changes, or a heightened sense of smell. None of these symptoms is specific enough to diagnose pregnancy.
It can be emotionally challenging to wait, particularly if you have experienced infertility, pregnancy loss, or uncertainty about your cycle. Try to be gentle with yourself. There is no behavior, symptom-tracking pattern, or pregnancy test schedule that can force the biology to declare itself earlier than it is ready.
- Consider taking a prenatal vitamin with folic acid if pregnancy is possible, unless your clinician has advised a different formulation.
- Avoid alcohol, smoking, vaping, and non-prescribed substances while trying to conceive or when pregnancy may be possible.
- Review prescription, over-the-counter, and herbal products with a healthcare professional, especially if you take medications for chronic conditions.
- Seek individualized advice if you have diabetes, hypertension, thyroid disease, epilepsy, autoimmune disease, kidney disease, or a history of ectopic pregnancy or recurrent miscarriage.
When to contact a healthcare professional
Week 3 is early, but medical guidance can still be valuable. Contact a healthcare professional if you have severe one-sided pelvic pain, heavy bleeding, fainting, dizziness, shoulder-tip pain, fever, or symptoms that concern you. These symptoms do not automatically mean something is wrong, but they deserve timely evaluation.
You should also seek tailored advice if you have a history of ectopic pregnancy, tubal surgery, pelvic inflammatory disease, recurrent pregnancy loss, or if you conceived with assisted reproductive technology. People taking medications with potential pregnancy implications, such as some anti-seizure medicines, anticoagulants, isotretinoin, certain blood pressure medicines, or immunosuppressants, should not stop treatment abruptly but should contact their prescribing clinician promptly for guidance.
If pregnancy is confirmed later, prenatal care usually begins with dating assessment, review of health history, medication and supplement counseling, screening discussions, and planning for appropriate follow-up. Early care is not about judgment; it is about support, risk reduction, and helping you make informed decisions.
Seek medical advice promptly if
- You have severe or worsening pelvic or abdominal pain, especially if one-sided.
- You experience heavy bleeding, fainting, dizziness, or shoulder-tip pain.
- You have a positive pregnancy test and a history of ectopic pregnancy or tubal surgery.
- You are taking medications and are unsure whether they are safe in pregnancy.
- You develop fever, severe vomiting, or symptoms that feel unusual or alarming.
Tools & Assistance
- Use a menstrual cycle or ovulation tracking app to estimate timing, while remembering it is not diagnostic.
- Keep prenatal vitamins, medication lists, and relevant medical history ready for a clinician visit.
- Contact an obstetrician-gynecologist, midwife, fertility clinic, or primary care clinician for individualized guidance.
- Use a home pregnancy test after a missed period for more reliable urine results.
- Seek urgent care or emergency services for severe pain, heavy bleeding, fainting, or concerning symptoms.
FAQ
Can I get a positive pregnancy test in week 3?
Sometimes, but it is often too early. hCG usually becomes detectable only after implantation begins, and urine tests are more reliable after a missed period.
Is implantation the same as fertilization?
No. Fertilization is when sperm and egg combine to form a zygote. Implantation occurs days later, when the blastocyst attaches to and begins to burrow into the uterine lining.
What is the difference between a morula and a blastocyst?
A morula is a compact ball of dividing cells. A blastocyst is a later fluid-filled structure with an inner cell mass that contributes to the embryo and an outer trophoblast layer that contributes to the placenta.
Should I change my medications if I might be pregnant?
Do not stop or change prescribed medications without medical advice. Contact your healthcare professional to review benefits, risks, and safer alternatives if needed.
Is light spotting during implantation normal?
Some people notice light spotting, but many do not. Heavy bleeding, severe pain, dizziness, or fainting should be assessed urgently by a healthcare professional.
Sources
- Cleveland Clinic — Fetal Development: Week-by-Week Stages of Pregnancy
- Mayo Clinic — Fetal development: The first trimester
- March of Dimes — Pregnancy Week by Week
Disclaimer
This article is for informational purposes only and does not replace professional medical advice, diagnosis, or treatment. Consult a qualified healthcare professional for personal guidance, especially if you have pain, bleeding, medical conditions, or medication concerns.















