Intro
The symptothermal method is a fertility awareness-based approach that combines basal body temperature (BBT) with cervical mucus observations, and often other cycle signs, to identify the fertile window with greater confidence than relying on a single sign alone. For people trying to conceive, it can help time intercourse around the days when pregnancy is biologically most likely. For people avoiding pregnancy, it can support decision-making about when abstinence or barrier protection is needed, though correct instruction and consistent use are essential.
This method can feel empowering because it turns daily body signals into a readable pattern. It can also feel demanding at first: cervical mucus changes may be subtle, BBT is affected by sleep and illness, and chart interpretation requires practice. A clinician or certified fertility awareness educator can help tailor the approach to your cycles, goals, postpartum or breastfeeding status, and any medical conditions that may affect ovulation.
Highlights
The symptothermal method combines two physiologic signals: cervical mucus, which reflects the estrogen-dominant fertile window, and BBT, which rises after ovulation under progesterone influence.
Mucus tracking is especially useful before ovulation because it can warn that fertility is approaching; BBT is most useful after ovulation because it helps confirm that ovulation likely occurred.
Using both signs can reduce uncertainty compared with BBT-only or mucus-only approaches, but accuracy depends heavily on correct daily observations, charting rules, and user consistency.
Irregular cycles, postpartum transitions, breastfeeding, perimenopause, polycystic ovary syndrome, shift work, fever, and disrupted sleep can make interpretation more complex.
The method is not a substitute for medical evaluation if cycles are persistently irregular, ovulation is unclear, or pregnancy has not occurred after an appropriate period of trying.
What the symptothermal method is
The symptothermal method is one of the fertility awareness-based methods of family planning. It uses a combination of cycle biomarkers rather than a single prediction tool. In its classic form, the method includes ]] and cervical mucus observations; some systems also incorporate cervical position, cycle length history, mid-cycle symptoms, or urinary hormone tests as supporting information.
The key idea is that fertility is not evenly distributed across the . Sperm can survive for several days in fertile-quality cervical mucus, while the ovum remains fertilizable for a relatively short time after ovulation. Therefore, the clinically relevant task is to identify the opening and closing of the as accurately as possible.
Professional organizations describe the symptothermal method as a combination approach because it uses ]] plus other signs and symptoms. This matters: BBT alone usually confirms ovulation only after it has happened, while mucus observations can indicate that the is beginning before ovulation. When the two signs tell a coherent story, chart interpretation becomes more reliable.
The physiology behind BBT and cervical mucus
BBT and cervical mucus are useful because they respond to ovarian hormones in different ways. Before ovulation, rising estradiol stimulates the cervix to produce mucus that is more abundant, slippery, stretchy, clear, or lubricative. This mucus helps sperm move through the cervix and survive in the reproductive tract. Many people notice a progression from dry or tacky sensations to creamy, wet, slippery, or egg-white mucus as ovulation approaches.
After ovulation, the corpus luteum produces progesterone. Progesterone has a thermogenic effect, meaning it slightly raises resting . In a typical ovulatory cycle, a appears after ovulation. The temperature shift does not predict ovulation in advance, but it can help confirm that the fertile phase has likely ended once specific charting criteria are met.
This division of labor is the strength of the symptothermal method. Cervical mucus acts as a forward-looking sign of approaching fertility, while BBT acts as a backward-looking confirmation sign. The combination helps distinguish a possible fertile pattern from a completed ovulatory event.
How combined tracking improves accuracy
Single-sign methods can be useful, but each has limitations. is vulnerable to confounders such as fever, alcohol, short sleep, travel, night waking, shift work, and taking the at inconsistent times. tracking can be affected by semen, lubricants, vaginal infections, antihistamines, hormonal medications, hydration changes, or difficulty distinguishing sensation from appearance.
Combining the signs helps create cross-checks. For example, if mucus becomes slippery and lubricative but no ]] rise follows, may not yet have occurred, or the ]] data may be disturbed. If a ]] rise appears but fertile-quality mucus continues, some charting systems advise caution until both the mucus peak and the ]] shift support the same interpretation.
The United States Conference of Catholic Bishops’ educational material emphasizes that, in symptothermal systems, is often treated as the primary fertility sign and BBT as a support or confirmation tool. This is practical: mucus helps identify when fertility is opening, and temperature helps confirm when it has likely closed. For couples trying to conceive, that means better timing around peak fertility. For couples avoiding pregnancy, it means fewer assumptions based on a single, potentially misleading sign.
What daily practice usually involves
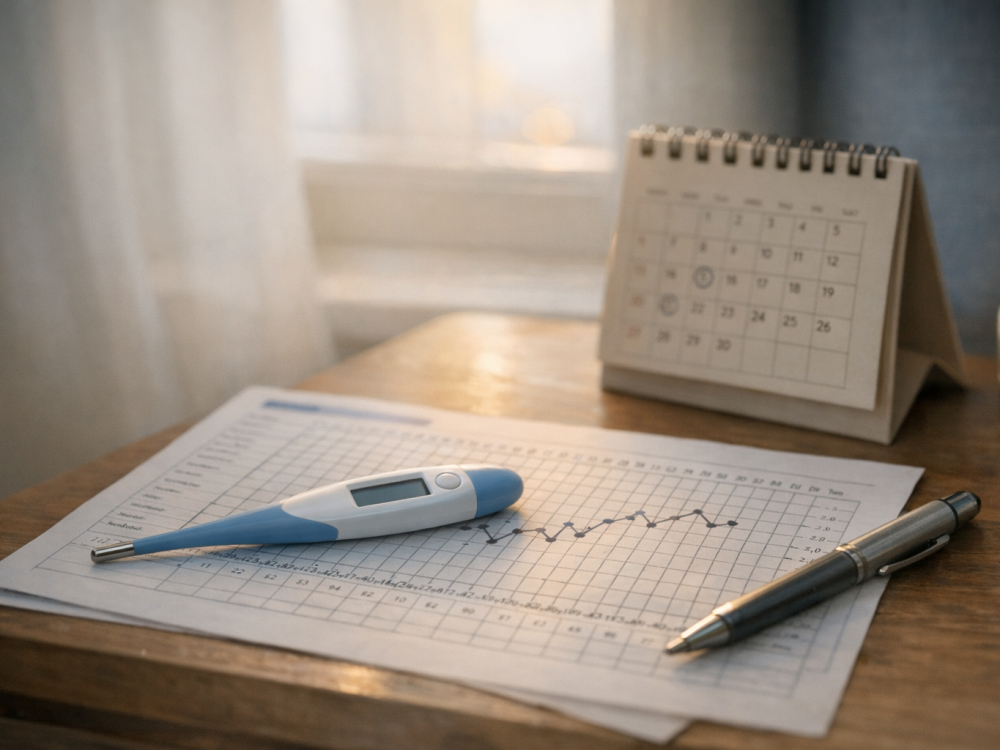
A typical symptothermal routine is simple in concept but benefits from consistency. BBT is usually measured immediately after waking, before getting out of bed, eating, drinking, or moving around much. Many users choose an oral, vaginal, wearable, or other basal thermometer method and keep the approach consistent across cycles. The absolute is less important than the pattern: the chart is looking for a sustained upward shift compared with the earlier, lower-temperature phase.
observations are made throughout the day, often by noticing vulvar sensation during normal activities and checking toilet tissue before or after urination. Charting systems vary, but categories commonly include dry, sticky, tacky, creamy, wet, slippery, stretchy, or egg-white. The most fertile sign is usually the last day of the most slippery or lubricative mucus pattern, often called the peak day, though it is identified retrospectively.
Many people chart using an app, paper chart, spreadsheet, or a fertility awareness instructor’s system. A practical daily record may include:
- Waking temperature and the time it was taken.
- Sleep quality, illness, alcohol intake, travel, or medications that may affect BBT.
- Mucus sensation and appearance, using consistent descriptive categories.
- Bleeding, spotting, pelvic discomfort, libido changes, or other cycle symptoms.
- Intercourse or insemination timing if trying to conceive.
The goal is not to achieve a perfect chart. The goal is to gather enough high-quality observations to interpret the cautiously and consistently.
Using the method when trying to conceive
When trying to conceive, the symptothermal method can help identify the days when is most likely to result in pregnancy. The highest-probability days are generally the days leading up to and the day of itself. Because BBT confirms after the fact, is especially valuable for timing. Slippery, clear, stretchy, or lubricative mucus often signals that is high and sperm survival is more favorable.
A common strategy is to have during days of increasingly fertile-quality mucus rather than waiting for the BBT rise. Once the shift is clear, the most fertile days for that cycle have usually passed. Over several cycles, charting can reveal whether mucus peaks and shifts occur in a consistent relationship.
Charts can also be useful clinically. If you see repeated cycles without a clear shift, very short luteal phases, persistent mid-cycle bleeding, or long unpredictable cycles, those patterns do not diagnose a condition by themselves, but they can provide helpful information for a clinician. People under 35 are often advised to seek evaluation after 12 months of trying, and people 35 or older after 6 months, but earlier consultation is appropriate for known reproductive conditions, irregular or absent periods, recurrent pregnancy loss, or other concerns.
Using the method to avoid pregnancy
For pregnancy prevention, the symptothermal method requires more conservative decision-making. Users must identify potentially fertile days and either abstain from vaginal or use a barrier method during that time, depending on the system and personal goals. The method’s effectiveness depends on correct use, including reliable observations, accurate chart interpretation, and consistent behavior during fertile days.
It is important to distinguish awareness from calendar-only prediction. Calendar estimate based on past s; symptothermal methods use current-cycle biologic signs. This can be especially helpful because can shift due to stress, illness, travel, postpartum changes, or other factors. However, current-cycle signs are only useful if they are observed and interpreted correctly.
If avoiding pregnancy would be medically or personally high-stakes, speak with a hehcare professional about the full range of contraceptive options. Fertility awareness may be a good fit for some people, but it is not ideal for everyone, especially when daily is not realistic or when cycles are difficult to interpret.
Limitations and common charting challenges
The symptothermal method is more informative than a single-sign approach, but it is not immune to ambiguity. BBT can be disturbed by febrile illness, insomnia, fragmented sleep, alcohol, jet lag, night shifts, and some medications. Wearable temperature devices may provide useful trends for some users, but they still need careful interpretation and may not follow the same rules as classic waking BBT.
Cervical mucus can also be difficult to interpret. Vaginal infections, arousal fluid, semen, lubricants, cervical procedures, breastfeeding, perimenopause, and medications that dry secretions can alter observations. Some people with polycystic ovary syndrome or irregular ovulation may experience multiple patches of fertile-type mucus before ovulation actually occurs, which can make the appear prolonged.
Learning with a qualified instructor can substantially reduce frustration. An instructor can teach standardized terminology, help identify disturbed temperatures, clarify peak mucus rules, and adapt guidelines for postpartum, breastfeeding, perimenopausal, or irregular cycles. Medical evaluation may also be appropriate if chart patterns suggest anovulation, thyroid disease, hyperprolactinemia, PCOS, or other endocrine concerns, but a chart alone cannot diagnose these conditions.
How to build confidence over several cycles
Most people need several cycles before the patterns become familiar. Early charts often feel messy because the user is learning both observation and interpretation. Try to focus on repeatable habits: take temperature at the same point in your waking routine, record mucus the same day rather than relying on memory, and note anything that might explain unusual readings.
It may help to review each completed cycle and ask: Did mucus become progressively more before the temperature shift? Was there a clear peak mucus day? Did the BBT remain elevated after the shift? Was the luteal phase reasonably consistent from cycle to cycle? These questions can help you recognize your personal pattern while staying cautious about outliers.
The method works best when it is approached as body literacy rather than a demand for perfection. Your cycle can vary and still be normal. If the data feel confusing, that is not a personal failure; it is a sign that you may need more support, better tools, or input.
When to get medical or professional guidance
- Seek urgent medical care for severe pelvic pain, heavy bleeding, fainting, fever, or a positive pregnancy test with one-sided pain.
- Consult a clinician if cycles are absent, persistently longer than 35–40 days, very irregular, or associated with significant pain or heavy bleeding.
- If avoiding pregnancy is essential, do not rely on self-taught charting alone until you have strong instruction and confidence in the method.
- Postpartum, breastfeeding, perimenopausal, and PCOS-related cycles often require specialized charting guidance.
- Fertility charts can inform care, but they cannot diagnose ovulation disorders or other medical conditions by themselves.
Tools & Assistance
- A basal thermometer or validated temperature-tracking device used consistently
- A paper chart, fertility awareness app, or spreadsheet that records both BBT and mucus
- Consultation with a certified fertility awareness educator or natural family planning instructor
- A gynecologist, reproductive endocrinologist, or primary care clinician for irregular cycles or fertility concerns
- A simple symptom log for sleep disruption, illness, medications, travel, and bleeding patterns
FAQ
Is the symptothermal method more accurate than BBT tracking alone?
It can be more informative because cervical mucus helps identify the fertile window before ovulation, while BBT helps confirm ovulation afterward. Accuracy still depends on correct observation, charting rules, and consistency.
Can I use an app to interpret my symptothermal chart?
Apps can organize data, but they vary in how they interpret fertility signs. If you are using the method to avoid pregnancy or have irregular cycles, professional instruction is safer than relying only on automated predictions.
What if my mucus and temperature signs do not match?
Discordant signs are common in disrupted or irregular cycles. Treat the chart cautiously, note possible confounders such as illness or poor sleep, and consider guidance from a fertility awareness educator or clinician.
Does a temperature rise prove that I ovulated?
A sustained BBT rise strongly suggests a progesterone shift after ovulation, but it is not absolute proof. Blood progesterone testing or ultrasound monitoring may be used clinically when confirmation is needed.
Can I use the symptothermal method while breastfeeding?
Some people do, but postpartum and breastfeeding cycles can be difficult to interpret because mucus patterns and ovulation timing may be irregular. Specialized instruction is strongly recommended.
Sources
- American College of Obstetricians and Gynecologists — Fertility Awareness-Based Methods of Family Planning
- United States Conference of Catholic Bishops — Sympto-Thermal Methods
- Natural Cycles — The Symptothermal Method Explained
Disclaimer
This article is for informational purposes only and does not replace medical advice, diagnosis, or treatment. Consult a qualified healthcare professional for personal guidance about fertility, contraception, cycle irregularity, or pregnancy concerns.















Please log in to leave a comment.